For many people, spring is in the air and finally, after the “mild” Omicron wave, it’s time to kick back, relax, and return to normal. Unfortunately, this view, promoted by the media, business, and government, has no basis in reality. If anything, the pandemic is accelerating as the mass infection of the Omicron wave and collapse of protections has unleashed a rogue's gallery of mutants that are making their presence known beginning with sublineages BA.2 and BA.2.12.1 and soon with one of their near relatives such as BA.4 or BA.5. It has already done so in the UK and Denmark, where excess deaths were elevated and hospitals were overrun while their governments downplayed the situation. Since April, cases and hospitalizations are again rising in the U.S.
In the United States, the adherents of the October 2020 Great Barrington Declaration, a call for a eugenic response to the pandemic, seem to have won. Some of those currently carrying out policies or appearing on TV to create the urgency of normal, such as Ashish Jha and Leana Wen, have previously disavowed the declaration’s strategy of herd immunity. Indeed, given the recent mid-flight revocation of the mask mandate on airlines in response to a nonsensical federal ruling (tellingly, the appeal by the government did not even request an emergency stay) the people rooting around and ripping out pandemic protections are edging ever closer to becoming literal gremlins on the airplane wing.
For the reality-based community, things feel hopeless now. No one is wearing masks and no one is social distancing. It's a common experience that simply wearing a mask invites criticism by perfect strangers. The CDC Director, Rochelle Walensky, said "...the scarlet letter of this pandemic is the mask." Nearly all protections have been dropped, quarantines are so short as to be useless, and testing is being cut back (exemplified by the end of free testing for the uninsured). A huge chunk of the U.S. will not get vaccinated. We've surpassed 1 million excess domestic deaths since the start of the pandemic with between 14 to 24 million globally.
On the CDC website, attempts are being made to dissuade people from looking at the original community transmission maps by claiming they are for “healthcare facility use only.” This is being done to guide people to view their new “Community Levels” standard map. In the new map, the term “low risk” has been so distorted that it includes transmission levels which were formerly termed “high risk.”[1]
The CDC attempts to dissuade website users from looking at the original transmission map.
Life is proceeding as "normal" while every moment in public, for anyone living in reality, is fraught with anxiety. It is like watching a dream world of sleepers play-act their lives. Astoundingly, even as a new more transmissible variant surges (and recombinant variants start to make their appearance), the dreamers remain asleep and this pattern continues across the western world.
Yet far from granting real freedom, this fantasy world traps the medically vulnerable more than ever as their margin of safety to travel outside vanishes. Children in schools are allowed to be repeatedly reinfected and parents are helpless as these infections recirculate within households. Future generations will look back on this period and condemn it as callously eugenic.
It's dark. It's bleak. Nonetheless, while we are in the darkest night and further dark days are ahead of us, things may be more hopeful in a year's time. The simple reason is we will learn, through pain, that this fool's paradise is not viable. Something will have to change.
The "let it rip" non-strategy will become recognized as non-viable because the material impact will be unsustainable. So far, we've lost a million more Americans than expected in two years. With waves of similar magnitude still hitting us every few months, can we continue to lose people at that rate? By 2030, we will lose five million souls or 1.5% of the 2020 population. Each person that dies leaves a blast radius that affects everyone they knew. It won't take many years before a majority of the population will know multiple people that have died and more that have Long COVID.[2] Just search for Long COVID on Twitter and you’ll find many patients that will loudly tell you that you don’t want it.
At this point it is becoming clear that the new variants are evolving faster than our vaccines can cope with and people are getting serially reinfected. Some of the people that get reinfected do better than the first time, but many also do worse, end up dead, in the hospital, or with Long COVID.[3] It won't be long before it begins to dawn on an increasing number of people that we are living in a harsher world. A healthy person only has to acquire a few small health ailments, as simple as getting a little older, and suddenly they are cut down.
Perhaps U.S. society, with its almost supernatural ability to normalize away the bad things that happen, will be able to do just that. However, there’s an economic dimension to this as well, and unfortunately, given our capitalist system and captured politics, this will drive the policy reaction in the absence of mass action by workers. In January of this year, Katie Bach at the Brookings Institute speculated that between 31 million working age Americans have had Long COVID, of which 4.5 million may have been sick at any one time, with about 1.1 million out of work due to their illness at any one time (or 0.6% of the US labor force).[4]
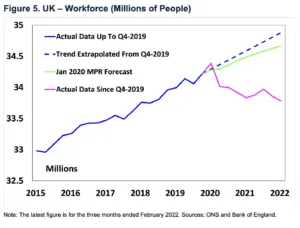
More recently in early May, the Bank of England revealed new data on the U.K. labor force that may show the beginnings of the economic effects of Long COVID. Monetary Policy Committee member Michael Saunders noted in a speech on the causes of record inflation that:
...since Q4-19, the economy’s potential output has fallen well below its previous trend.
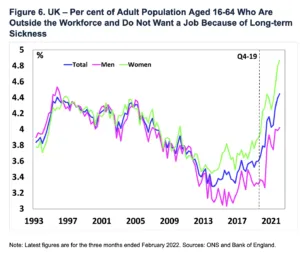
The workforce has shrunk by 440,000 people.… Since Q4-19, the number of people aged 16-64 years that are outside the workforce and do not want a job has risen by 525,000 (1.3% of the 16-64 age population). This largely reflects increases in long-term sickness (roughly 320,000 people) and retirement (90,000), with smaller contributions from lower participation among students (65-70,000) and short-term sickness (30-35,000 people). The share of the 16-64 population who are outside the workforce and do not want a job because of long-term sickness is a record high, with an especially sharp rise among women. I suspect much of this rise in inactivity due to long-term sickness reflects side effects of the pandemic, for example Long Covid and the rise in NHS waiting lists.
As disability grows with serial reinfections, it's possible that fewer workers will be available for full-time shifts, and some of them may work more slowly. This will be one more long term economic drag on an economy that is in an era of anemic growth and consumer inflation.
How much economic damage can the government tolerate before they react? A crucial upper bound is set by whether GDP growth remains positive. If the economy chronically stagnates or net value is destroyed, capitalism will become delegitimized as it will be working with a fixed pie. This means life will get materially worse for everyone but the upper class since capitalism mechanically produces inequality. The severity of the problem will dictate the amount of political delegitimization.
There may also be a higher threshold of action as, since 1990, the U.S. empire spends about 3-5% of GDP annually on the military.[5] If production or consumption falls sufficiently, it will be impossible to maintain military spending without radical changes as every bullet purchased detracts from the civilian economy. With reduced military spending, the influence of the global U.S. empire will shrink, perhaps catastrophically (in the view of its planners). These considerations may become relevant sooner rather than later given the burgeoning U.S. proxy war with Russia.
Yes, we will learn through pain. Nonetheless, we are also witnessing the large-scale evolution of twin processes of grief and social learning.
We’ve seen many delusions appear over the course of the pandemic. The denial that obvious public health measures like masking or closing schools and businesses would be effective. The indulgence in snake oil cures like hydroxychloroquine, Ivermectin, and vitamin D. The denial that COVID is airborne, or that Omicron was “mild” (it wasn’t). The aggressively pedaled ideas that the vaccine would end the pandemic or that the vaccine was the real cause of illness; that COVID deaths were faked, that the deaths were miscategorized at mass scale (died “from” or “with”) to inflate the pandemic. We’ve even seen the granddaddy of them all: “COVID is over.” New deeply and powerfully held delusions have continuously appeared and spread faster than the virus.
At this point, it seems many have turned to denial, even though it hurts both themselves and others. They lash out when they are reminded that things are not okay and that they're hurting those around them. That's why many become so aggressive towards the lone person in the room wearing a mask.
Since the pandemic and its reminders of mortality are not going away, we should expect to see people continue to cycle through the five stages. Eventually, we can find a more plausible way, hopefully a rational and life preserving way, of coping with our new world.
Another part of the problem is the social learning component. Many are struggling to cope with a world that isn't following the movie script they had in their head. This is rather important; Americans belong to few civic or political organizations, so they don't solve problems deliberatively with their fellow citizens. Instead, since most of them have TVs or computers, they are mainly organized via their reactions to media.
In early 2020, the media began talking about a new mysterious pandemic that rightly scared the daylights out of the public. People were frightened enough that they did things that previously seemed impossible, such as staying home and working remote, revising their view of the people that staff stores as essential workers, closing businesses, and forcing the government to perform limited and therefore ineffective lockdowns. The roads were cleared and wild animals walked out onto American streets unopposed like a science fiction movie.
Just as importantly, their expectations were set when the media talked about "flattening the curve" but not about "suppressing the pandemic." Though it was later criticized on its methodology, a group at the Imperial College in London led by Dr. Neil Ferguson predicted the deaths of about 1.2 million Americans in the best case scenario with a peak death rate of 56,100 per day assuming no mitigations.[6] We’ll never know if they were right on the peak rate since we did put a partial suppression strategy into place. The real rate was about 3,375 (7 day rolling average), but the estimate was pretty close on the total number of dead after two years (which is still rising).[7]
The unexpectedly large reaction of the public and nearly every institution blunted what could have been an even more monstrously huge and deadly wave. At that time, the primary historical reference for the pandemic was the 1918 H1N1 influenza pandemic which is suspected to have originated at a Kansas army installation and shipped out to the world in WW1.
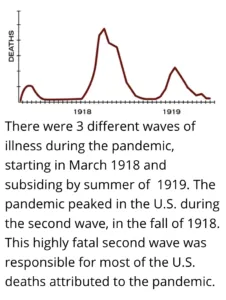
The 1918 influenza pandemic, which occurred in three major waves, had an unusual age-severity curve that yielded huge numbers of dead young people in the prime of their lives.[8] The second wave was most prolonged and deadly. The first and smallest wave was seen in March 1918 and subsided by summer. The flu disappeared and reappeared after mutating into a monster on the battlefields of WWI.[9] In the U.S., the second wave lasted from October to early-December 1918. The third wave hit in late January 1919 and lasted until part way through the spring. Then, the H1N1 flu mysteriously petered out and disappeared (until scientists reconstituted it in 2005 under BSL3 conditions to study what made it so unique).[10] It then mysteriously reappeared as a seasonal flu.
A common hypothesis for why this happened was that H1N1 was not able to adapt quickly enough and hit an immunity wall in the survivors, and thereafter was unable to propagate.[11] It then mutated over time to become a milder disease. However, no one really knows what happened. Why didn't the virus simply mutate to become immune evasive? Why would its modern incarnations be milder? The reasons probably have something to do with influenza's biology, the human immune system, and sheer contingency.
The flu pandemic was intense, scary, and deadly but the most visible part lasted less than a year. It was a relatively recent event that seemed to roughly match our circumstances. Thus, this event drove expectations even though the pathogen was a different species. With this historical context in mind, people acted their roles to a reasonable degree throughout 2020. They hid when the danger was near and went out when the danger was less.
Our mental script consists of more than just the precedent of past events. It also consists of fictional plotlines amalgamated from zombie movies, TV shows, and a handful of pandemic-themed films such as Outbreak (1995), 12 Monkeys (1995), and The Andromeda Strain (1971, 2008 TV-remake). The most realistic of the bunch, Contagion (2011), was modeled on the comparatively limited 2003 SARS and 2009 Influenza epidemics.
In these movies, how did the pandemic end? (decades old spoilers ahead):
In zombie movies, usually the survivors either die, reach a fortified human settlement, kill all the zombies, or find a cure. In Outbreak (1995), a lethal virus is spread by an illegal pet monkey imported into the U.S. The government attempts to drop a thermobaric explosive on a quarantined California town (after having done so previously in Africa). They are stopped by a heroic military scientist from Ft. Detrick that finds a cure in monkey antibodies. (Parts of this movie almost happened in reality in Dansville, PA very recently.)[12] In 12 Monkeys (1995), Bruce Willis is sent back in time to trace the spread of a virus that forced humanity to live underground. He tries to stop the virus’ origin, a bioterror plot at an airport, but fails because you can't change time. In the Andromeda Strain movie (1971), a highly lethal alien organism captured by a satellite is studied in an underground lab after wiping out a small New Mexican town. It escapes, but humanity is saved when it mutates to eat plastic and becomes harmless. In the Andromeda Strain TV show (2008) the writers alter the story and the humans save the day by using a sulfur-eating bacterium from a deep-sea thermal vent to fight it. In Contagion (2011), a highly realistic movie, a fictional lethal zoonotic virus called MEV-1 spreads from Hong Kong. It transmits via respiratory droplets and fomites (by touching infected surfaces). The virus spreads around the world and piles up bodies. The film shows how the government, especially the CDC, responds by encouraging social distancing. Unlike in other films, the situation isn't fully resolved at the end of the movie. A vaccine is introduced but it takes a while to ramp up production, so a lottery system is used to distribute it. Near the end of the movie, scientists are shown putting a sample of MEV-1 on ice, but resolution is quickly undercut. The protagonist finally allows a boy that's interested in his daughter into his living room for a senior prom, but only after checking his vaccine card.
This selection of movies featured the following resolutions: IV antibodies, a vaccine, the organism mutates to become non-lethal, we fight it with another organism, and humanity lives underground indefinitely. Nonetheless, I surmise that due to the fact that movies end after an hour or two, regardless of how they resolve, people walk away with the impression that pandemics end in a tidy fashion.
So putting what we've learned together, the plot of our real-life pandemic story looks something like this. A novel virus appears in 2020. Based on the 1918 flu, we generally expect it to last for a few months. After the first wave, the more historically literate point out that there were actually two big waves in 1918, so many people accept that winter 2020-2021 will be bad (it was). In January 2021, an apparently highly effective vaccine is introduced far ahead of public expectations due to the federal government’s Operation Warp Speed which features the new mRNA technology. Everyone debates the safety of the new technology, and many people (but not enough) get vaccinated. This is the point at which the movie is supposed to end.
However, the movie doesn't end. The plot devolves into a mess. A culture war develops between pro- and anti-vaccine camps. Vaccination rates peak in April and collapse to a crawl in July 2021. As this happens the virus mutates (Alpha, Beta, Delta, and others) to become more severe, more transmissible, and more immune evasive, like a bad sequel. Unfortunately for the pro-vaccine crowd, the new heightened transmissibility of Delta will require something like 90% of the population to be fully vaccinated to achieve "herd immunity" (currently 67% are fully vaccinated).[13]
Furthermore, we start to discover that the vaccine's protection against infection is temporary (though hospitalization and death are mostly protected against). Our heroes are in trouble. In Fall 2021, boosters are rolled out as the Delta wave begins, but only a third of Americans will take them by April 2022.
Then, in November 2021, the Omicron BA.1 variant appears, which is both much more transmissible and more immune evasive, but somewhat clinically less severe and so is termed "mild." It will kill over 100,000 Americans in a very short time. The word "mild" is repeated relentlessly by politicians and the media.[14] Later, it will be shown that after controlling for vaccinations, demographics, and comorbidities, Omicron BA.1 is not intrinsically milder. Interestingly, "mild" was the terminal point of both the 1918 pandemic and The Andromeda Strain (1971) movie. Finally, we're back on script. People think the pandemic is over because, in cinematic terms, it should be and every authority figure is saying so! It doesn’t help that the increased transmissibility helps create a sense of inevitability.
This set of circumstances is then readily exploited by politicians to aid their friends’ money making schemes. They try to erase the pandemic from the public consciousness to keep the U.S. consumer base consuming, the workers producing, and the imperial arms rolling off the assembly line.
Unfortunately, since the virus is still evolving, a new Omicron subvariant wave is beginning. The movie magic will inevitably come to an end when people’s social circle starts dying or getting disabled again. Unfortunately, it may take a few cycles of reinfection to dispel the illusions promoted by the government and its allies.
It's somewhat comforting to learn this situation isn't entirely novel. In 1918, politicians downplayed the influenza pandemic too. In "The Threat of Pandemic Influenza: Workshop Summary" from the Institute of Medicine (US) Forum on Microbial Threats 2005, the authors wrote:
Routinely, as influenza approached a city or town... local officials initially told the public not to worry... When influenza first appeared, officials routinely insisted at first it was only ordinary influenza, not the Spanish flu. As the epidemic exploded, officials almost daily assured the public that the worst was over...
This pattern repeated itself again and again. Chicago offers one example: Its public health commissioner said he'd do “nothing to interfere with the morale of the community… It is our duty to keep the people from fear. Worry kills more people than the epidemic.
That idea—“Fear kills more than the disease”—became a mantra nationally and in city after city…
In Philadelphia, when the public health commissioner closed all schools, houses of worship, theaters, and other public gathering places, one newspaper went so far as to say that this order was “not a public health measure” and reiterated that “there is no cause for panic or alarm.”
But as people heard these reassurances, they could see neighbors, friends, and spouses dying horrible deaths.
In Chicago, the Cook County Hospital mortality rate of all influenza admissions—not just those who developed pneumonia—was 39.8 percent. In Philadelphia, bodies remained uncollected in homes for days, until eventually open trucks and even horse-drawn carts were sent down city streets and people were told to bring out the dead. The bodies were stacked without coffins and buried in cemeteries in mass graves dug by steam shovels.
This horrific disconnect between reassurances and reality destroyed the credibility of those in authority. People felt they had no one to turn to, no one to rely on, no one to trust.[15]
While COVID-19 is not as lethal as the pandemic flu was, it’s nonetheless eerie how similar this aspect of the 1918 response, where public officials emphasized that fear was worse than the disease, is to our present day. It’s even more unsettling when we consider that it’s sometimes suggested that if COVID-19 were more lethal, our society would respond more rationally. Day by day, reports trickle in, both from the scientific and mainstream press, of the damage the disease wreaks at every level of severity on the vasculature, brain, heart, pancreas, kidneys, and other organ systems. Because this disease process is slower and more subtle than piles of body bags thawing in mobile morgues, it will take more time for people to process it.
Rarely but poignantly is a comparison made with the ongoing AIDS pandemic. The AIDS pandemic featured a deadly novel virus that forced us to change our practices around sex and handling blood permanently, an abused minority population, a simultaneously malign and incompetent government response, and a treatment regime that took many years to figure out. The AIDS virus didn’t kill immediately and so the argument was made that people died with HIV and not from HIV.
However, in time, we discovered that HIV simply damages the body enough for other problems to become lethal (in HIV’s case, usually cancer or opportunistic infection). It is possible that this pattern will repeat for the novel coronavirus as well. If SARS-2 damages your organs and you die of diabetes, liver failure, or kidney failure years later, the causal relationship remains. If you acquire such brain fog as to be unable to work productively and die of poverty in a ruthless capitalist economy, was it not the infection that incited a spiraling sequence of events?
We still live with HIV. HIV patients do so literally. We had to adapt, and it took years of activism by the LGBT community to force the government to do its job. Indeed, one of the original officials they lobbied was Anthony Fauci! HIV never got milder (one strain became more severe).[16] We never got a vaccine. We never got a cure. We developed effective treatments and got smarter. SARS-CoV-2 is a very different virus from HIV. Unfortunately, we may nonetheless be living with it for some time. We will have to adapt to it as well.
I expect our environments will become safer with enhanced ventilation. Masking will again become accepted during outbreaks – Asians learned to do so after the 2003 SARS outbreak. Second generation medications and vaccines will be developed. Compensation for victims will be procured. However, these things will take both time and workplace activism that can hold the ruling class accountable by denying them access to our labor. In the meantime, it is important to make clear that you are not crazy, no matter what people say. Protect yourself and those around you as best you can. Wear masks, get vaccinated, take tests, and avoid crowded indoor areas. Stage walkouts and work stoppages to demand protections be put in place.
Form or join a union that will fight for your bodily and financial protection. If Amazon workers could do it, opposed by the most powerful people in the world, so can you. Start organizing to make the changes. The most hopeless time of the pandemic is right now. Eventually the wheel will turn.
Liked it? Take a second to support Cosmonaut on Patreon! At Cosmonaut Magazine we strive to create a culture of open debate and discussion. Please write to us at submissions@cosmonautmag.com if you have any criticism or commentary you would like to have published in our letters section.
- The meaning of the new map appears to be an indicator as to whether there “will be a hospital bed available for you” rather than “will I get COVID”, or in other words, a complete surrender. The term “Community Levels” is also squishy. It’s not clear what a “community level” means and so can be defined arbitrarily. ↩
- Long COVID, defined as one or more persistent symptoms, affects 20-25% (1 in 4-5) of all singly infected people according to CDC MMWR. A “rare” medical condition is defined in the European Union as affecting 1 in 2000 people. ↩
-
A recent study found that vaccination only reduced the incidence of Long COVID by 15% (Hazard Ratio 0.85) in breakthrough infections. Vaccination also prevents many infections, which means overall vaccines do better than those figures. However, breakthroughs are increasingly frequent.
Al-Aly, Z., Bowe, B. & Xie, Y. “Long COVID after breakthrough SARS-CoV-2 infection.” Nat Med (2022). https://doi.org/10.1038/s41591-022-01840-0
“Compared to people with SARS-CoV-2 infection who were not previously vaccinated (n = 113,474), people with BTI exhibited lower risks of death (HR = 0.66, 95% CI: 0.58, 0.74) and incident post-acute sequelae (HR = 0.85, 95% CI: 0.82, 0.89).” ↩
- https://www.brookings.edu/research/is-long-covid-worsening-the-labor-shortage/. ↩
- https://data.worldbank.org/indicator/MS.MIL.XPND.GD.ZS?locations=US. ↩
- “Report 9: Impact of non-pharmaceutical interventions (NPIs) to reduce COVID-19 mortality and healthcare demand” by Ferguson et al. (March 16, 2020). ↩
- https://ourworldindata.org/covid-deaths. ↩
- https://www.cdc.gov/flu/pandemic-resources/1918-commemoration/three-waves.htm. ↩
- https://www.cdc.gov/flu/pandemic-resources/1918-commemoration/pandemic-timeline-1918.htm. ↩
- "The Deadliest Flu: The Complete Story of the Discovery and Reconstruction of the 1918 Pandemic Virus" https://www.cdc.gov/flu/pandemic-resources/reconstruction-1918-virus.html. ↩
- https://time.com/5894403/how-the-1918-flu-pandemic-ended/. ↩
- “Questions Remain After Highway Crash Involving Monkeys” by Michael Levenson (February 1, 2022) https://www.nytimes.com/2022/02/01/us/cdc-monkeys-pennsylvania-truck-crash.html. ↩
- https://cosmonautmag.com/2021/12/covids-hidden-cost-why-living-with-the-virus-is-not-an-option/; https://www.nytimes.com/interactive/2021/us/covid-cases.html. ↩
- Though not the socialist daily WSWS (with whom the author has no affiliation and even the occasional disagreement) which has generally had good and timely coverage of COVID-19: “Omicron is not “mild”” on Jan. 7, 2022. ↩
- “The Threat of Pandemic Influenza: Workshop Summary” (2005) https://www.ncbi.nlm.nih.gov/books/NBK22148/. ↩
- Wymant et al. “A highly virulent variant of HIV-1 circulating in the Netherlands“ Science. February 2022. https://www.science.org/doi/10.1126/science.abk1688. ↩